|
STREPTOCOCCUS PYOGENES
(LANCEFIELD GROUP A)
The majority of β-haemolytic streptococci causing infections in man
belong to group A and are given the species name Streptococcus pyogenes
which is normally found in the throat or nasal cavity in a proportion of
apparently healthy people (carriers).
Morphology :
Gram positive cocci, 0.7-0.9 µm in diameter, occurring in chains of varying length, non-motile, non sporing and some are capsulated in very young cultures. 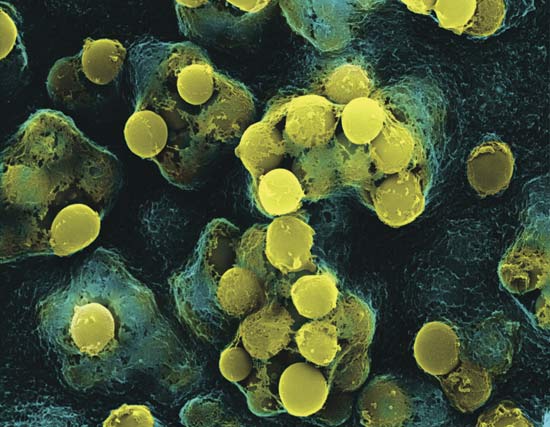
Cultural Characters :
Facultative anaerobe, optimum temperature for growth 37°C. Does not grow on nutrient agar on MacConkey's agar. Grows on blood or serum agar. Clear often wide zone of haemolysis surrounds colonies on horse or sheep blood agar. 
Biochemical Activities :
Streptococcus pyogenes is catalase negative and sensitive to bacitracin which could be used for its identification in place of antigenic study.
Antigenic Structure :
β-haemolytic streptococci can be divided into 20 different serologic groups according to C antigen and certain groups can be subdivided into types according to M and T protein-antigens: 1. Group specific cell wall antigen (C antigen): This carbohydrate is contained in the cell wall of many streptococci and forms the basis of serologic grouping (Lancefield groups A-H and K-V). 2. M protein: This substance is closely associated with virulence of group A streptococci and occurs chiefly in organisms producing matt or mucoid colonies. Group A streptococci can be further subdivided into over 80 Griffith's serotypes (types are assigned Arabic numbers) on the basis of specific M protein antigens of cell wall. It is antiphagocytic, and immunogenic. 3. T protein: It is another surface antigen. This antigen has no relationship to virulence of streptococci. T substance permits differentiation of certain serotypes of streptococci by agglutination with specific antisera. 4. R protein: It is another surface antigen, present in few group A serotypes, its signification is unknown.
Toxins
And Enzymes :
More than 20 extracellular products that are antigenic are elaborated by group A streptococci, including the following: 1. Streptokinase (fibrinolysin): It tranforms the plasminogen of human plasma into plasmin, an active proteolytic enzyme that digests fibrin and other proteins. 2. Streptodonase (streptococcal deoxyribonuclease): Depolymerizes DNA. Mixture of streptodornase and streptokinase help to liquify exudates and facilitate removal of pus and necrotic tissue, antimicrobial drugs thus gain better access and infected surfaces recover more quickly. 3. Hyaluronidase (spreading factor): Splits hyaluronic acid, an important component of the ground substance of connective tissue. Thus, hyaluronidase aids in spreading infecting micro-organisms. 4. Erythrogenic toxin: Only strains of group A streptococci that produce this toxin can cause the rash of scarlet fever. Production of this toxin is determined by specific bacteriophage in the lysogenic state. 5. Diphosphopyridine nucleotidase: This enzyme may be related to the organism's ability to kill leucocytes. 6. Haemolysins: β-haemolytic group A streptococci elaborate two haemolysins (streptolysins). (a) Streptolysin O: It is inactivated in the presence of oxygen (oxygen labile), it is antigenic and antibody to streptolysin O develops after infection. An antistreptolysin O (ASO) serum titre in excess of 160-200 units is considered abnormally high and suggests either recent infection with streptococci or persistently high antibody levels due to an exaggerated immune response to an earlier exposure in a hypersensitive person. ASO titre helps in the diagnosis of rheumatic fever. (b) Streptolysin S: It is not inactivated by oxygen (oxygen stable), it is responsible for the haemolytic zones around streptococcal colonies on blood agar plate incubate aerobically. It is not antigenic.
Pathogenesis :
I. Inflammatory and suppurative conditions: The most common infection due to Streptococcus pyogenes is tonsillitis. Other diseases are scarlet fever, cellulitis, erysipelas, impetigo, puerperal sepsis, otitis media, acute endocarditis and wound infection. II. Streptococcal toxic shock syndrome: It is a fulminant disease caused by certain strains of streptococcus pyogenes characterized by soft tissue infection together with shock, bacteraemia and multi-organ failure. III. Post-streptococcal infection: It follows an acute group A streptococcal infection, there is a latent period of 1-4 weeks, after which glomerulonephritis or rheumatic fever occasionally develops. Nephritis is more commonly proceded by infection of the skin, while rheumatic fever by infection of the respiratory tract. 
Laboratory Diagnosis :
They includes: 1. Antigen detection tests: Several kits are available for rapid detection group A streptococcal antigen from throat swabs. 2. Identification of β-haemolytic streptococci: from the patient's blood or exudates,
Specimens :
Specimens to be obtained depend upon the nature of the streptococcal infection. A throat swab, pus or blood for culture.
Smears :
Gram-stained smears from pus often show gram positive cocci singly or in pairs. Smears of throat swab are rarely of value.
Culture :
Specimens are inoculated onto blood agar plates and incubated under both aerobic and anaerobic conditions. After 24 hours incubation, plates are examined for β-haemolytic translucent colonies. Anaerobic incubation improve haemolysis.
Identification :
(a) Bacitracin sensitivity: The isolated β-haemolytic streptococci can be proved to belong to group A by testing its sensitivity to a bacitracin disc. (b) Grouping of β-haemolytic streptococci: Various methods can be used for grouping streptococci (e.g. precipitation test, latex agglutination, ELISA, gel diffusion , and fluorescent antibody test) using specific antisera. (c) Typing group A streptococci: Can be made for epidemiological purpose using specific antisera againt M and T protein antigens.
3. Serologic tests:
The patient's serum is examined for a rising titre of antibody to one or more streptococcal antigens e.g. the anti-streptolysin O (ASO).
In-Vivo Neutralization
Reaction :
In case of scarlet fever, Schultz-Charlton test can be used to help in the diagnosis, while Dick test can be used to measure the immune status of person to erythrogenic toxin.
Dick test :
0.1 ml of the toxin is injected intradermally in one forearm, in the other, inactivated toxin (boiled for one hour) is injected as a control. If the person is not immune (no antibodies in the serum) an erythematous rash more than 10 mm in diameter appears within 8-24 hours. Negative test indicates immune status (antitoxin present in the serum). Antitoxin to erythrogenic toxin prevents the rash of scarlet fever, but does not interfere with streptococcal infection.
Schultz-Charlton
reaction :
Is used to help in the diagnosis of scarlet fever. Injection of the erythrogenic antitoxin into the rash will cause the redness to blanch if the toxin is neutralized. |
||||||
|
||||||

STREPTOCOCCUS PYOGENES
|
||||